K-SLP Research & Clinical Excellence
A Message from Nancy R. Kaufman, MA, CCC-SLP

Parents understandably want the very best for their children, and they are inundated with information about different types of therapy. In the search for the best approach, we often look for proof, and I am often asked about the research behind the Kaufman Speech to Language Protocol (K-SLP). We’d like to take some time to address this.
I value research and respect the professionals whose intentions are to determine what constitutes best practices for those with childhood apraxia of speech (CAS). However, it is important to consider the expertise of the clinician who is on the front lines, working with children daily, yielding years of experience with what we know works. Clinical experience is just as important as research.
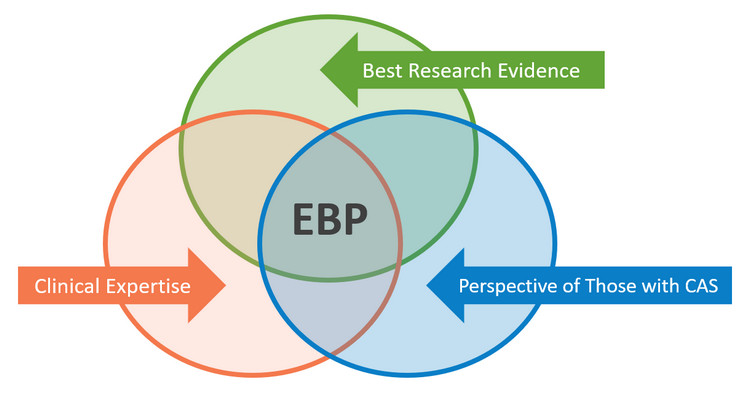
The best evidence informed practice consists not only of researched evidence, but also of clinical expertise and the parent’s satisfaction of their child’s treatment:
Research on Childhood Apraxia of Speech
Here are some thoughts about research from our friends at Apraxia Kids.
Apraxia Kids
We also must ask ourselves, since research is an ongoing process how do we address the needs of children who may not be benefiting from a protocol with a higher level of research. This is a real concern and one that needs to be addressed. Here is Apraxia Kids’ position on this matter.
Apraxia Kids
With that in mind, we must understand that just because an approach has been researched with positive results does not mean approaches that have not been researched are at all inferior. What is important is that the approach follows best practices found within the most-current research.
The K-SLP was developed in the early 1980’s. This was during the time when research was just beginning regarding CAS. However, it is exciting to find that the K-SLP has been following the most current research on CAS since its inception. The K-SLP has never been a stagnant method. It continues to evolve whenever new research calls for changes or updates in how techniques are implemented.
The K-SLP is rooted in the principles of behavior learning, which have existed since the 1950s and mirror current research for the principles of motor learning:
- Establishing a behavior that doesn’t exist
Example: gaining vocal imitation or gaining an increase of isolated vowels or consonants - Improving upon a behavior that does exist
Example: helping children to have improved speech clarity to use functionally for expressive language - Extinguishing behaviors that are interfering to the process
Example: adding schwa, adding extra vowels or syllables - Behavior management
Example: eliminating behaviors interfering with progress in therapy
Specifically for CAS, the K-SLP methods include the following:
- Choosing target words on the basis of the child’s vowel and consonant repertoire and determining best approximations toward perfection of words that will provide the child with functional communication, starting with single words
- Implementing and fading multisensory cues (visual, auditory, tactile/proprioceptive)
- Implementing different practice schedules (massed, distributed, etc.) to facilitate target words and phrases
- Implementing errorless teaching (cueing before failure)
- Mixing and varying tasks to avoid teaching overgeneralization
- Using reinforcement strategically, according to the child’s interests and needs
- Coaching parents and caregivers through play and natural environment teaching
The K-SLP materials were created out of a necessity arising from clinicians who have been implementing these methods. Although the materials were originally created for clinicians, they have been found to be effective for parents when instructed by the SLP. Coaching parents through play and the natural environment is inherent to the K-SLP.
Children from the United States and over a dozen other countries have become effective vocal communicators with the K-SLP methods. While we continue researching treatment approaches, we are all attempting to clearly define CAS. As a clinician I have looked at speech-motor skills on a continuum and do feel there are levels of severity for CAS. I maintain that this will be validated.

K-SLP Success Stories
Below you can watch videos of children with varying degrees of CAS who have made significant progress. This is due to the team effort between me and their SLP teams, parents, family members, and caregivers…as well as the children's own hard work!
Jason’s Progress
John O’s Progress
John S’s Progress
Josie’s Progress
View More Videos
Click below for the before-and-after videos of more kids!
We will be posting a few additional videos per month. If you have not seen your child’s videos, it is possible that they are scheduled to be showcased at a later time, or we may not have been able to locate early videos.
We would love to hear about your child's success with the K-SLP methods. Please contact us.